Posts Tagged ‘physical therapy’
11/8/2016 EDS – What is it and do I have it?
Posted by admin in My History on November 13th, 2016
EDS stands for Ehler’s Danlos Syndrome. And it’s been a recurring phrase in my family ever since my little brother got diagnosed about fifteen years ago. According to the Ehler’s Danlos Society website (http://ehlers-danlos.com/what-is-eds/), EDS is an hereditary syndrome that effects the connective tissue in the body. Although there are many types, the most common “is known or thought to alter the biology of collagen…. (the most abundant protein), which can lead to multi-systemic symptoms.” EDS has been identified as having six different types, all of which have genes associated with them – except for the hypermobile syndrome.
Why bring this up, now?
If you’ve been reading along, you’ve noticed that I go to the physical therapist at least twice per year. Also, I cannot follow a recommended training program for running (as in prepare for a marathon in 6 months! NO WAY! I’ve been trying to go farther than a 10K for four years with not so much luck or success), and I cannot train with anyone else because they inevitably progress faster than I do. After working on triathlons, running and cycling races and rides, I finally thought that I should find out if I, too, have EDS. Also, if I do have it, am I doing everything I should be doing? Or am I overdoing it by training too much?
Thus, last Tuesday, I walked into a the geneticists office for my long awaited appointment (I scheduled my November appointment in April of this year) wondering if they were going to look at me and tell me I needed to “Suck it up, Buttercup. This is normal.” Or if they would tell me there was a reason for all the PT.
Now, what happens at a genetic appointment? That’s a great question. Seeing as how I was at a research hospital at a major university who is top ranked in the nation, I had not one, but two to four people in the room at any given time. To start, two people entered the room for my initial intake, a woman with her PhD in genetics (I cannot remember if she was a post-doc, intern or full doctor because I was pretty nervous at this point) and a man who works in the lab, but wanted to see the office side of the process (he tested the DNA for the genes associated with EDS). The woman did the interviewing asking me family history (who else was flexible with soft skin, etc.) as well as my symptoms. She then had me stand up and walk, flex my knees back, flex my elbows, and touch my thumb to my wrist, which I didn’t know I could do, but was able to on my left hand – weird!
At some point, she said, “Do you have a good physical therapist?”
I almost cried.
Why? Because all of my normally developing friends have at some point or another asked or questioned why I have to go to the physical therapy so very much. And I can only reply because my Posterior Tibial Tendon is inflamed again because I did too much too fast (which means that I tried to keep up with that person’s training regimen). Or my right knee (patellular tendonitis) is inflamed. Or my right shoulder is inflamed. Or my left adductor is inflamed. You name it, it’s been inflamed due to repetitive stress injury.
So, when I walked in and the geneticist looked at me and confirmed that a PT is not only helpful but necessary, I finally felt like I wasn’t making it all up.
Flashback: When I was about 8 years old, every time my mom and I went shopping at an outlet mall or other LARGE area of concrete flooring, my feet would nearly bring me to tears because they hurt so bad. My mom did not always believe me, and sometimes I thought that maybe I was making up the pain – maybe this was what everyone felt, and they just handled it better than I did. Maybe I was just a cry baby. “Suck it up, Buttercup.”
However, in one fowl swoop, this doctor had made me realize that I had not and I am not making any of it up. It’s for real. Running for longer than three miles hurts, while run/walking for five miles is GREAT! Cycling is GREAT! As long as I have not inflamed my PTT from running too far first. Taking a six week training class to help improve run time is a disaster. Working out with a group to train for a triathlon, not always a good idea. But working out with a trainer who makes a program just for me is GREAT! Etc.
Back to the appointment, the initial geneticist and lab guy left and returned a few minutes later with Dr. Byers, the genetic guru, and another woman (genetic counselor). Dr. Byers went over an abbreviated version of the previous interview, then he examined my skin, felt for muscle tone (backs of my shoulders were a little flat – nothing some swimming wouldn’t correct), and asked me to walk. We talked about my club feet (could be indication of EDS or could have been due to my mom’s uterous being twisted), my small upper pallet (I have heard that this could be a trait, and both me and my brother had it – although he didn’t really seem to be too impressed with that trivia), and my yoga abilities.
Then, Dr. Byers said that I am definitely hypermobile, but there is no genetic test for it. He would not say that I am full on EDS, but there is definitely hyper flexibility in my joints that can lead to early onset arthritis and other difficulties as I age. He also said that my strength training was phenomenal. (Yay!) He then told me that I should swim because it is the BEST activity for joints around. In addition, he regularly swims at my neighborhood pool. Really? Great! I used to swim, but just haven’t in a while because getting back in the habit is really difficult. Blah, blah. Suck it up, Buttercup! Ready for the pool? 🙂
Now, don’t think that I am disappointed in having a non-gene specific hypermobile syndrome. Quite the opposite. By having this type, I am not in danger of having the Vascular Type, which can cause ruptures in artieries, veins and other organ tissues; nor the Arthrochalasia Type, which involves lack of muscle tone; nor do I have a type associated with gum disease and dental problems.
No, I am hypermobile. AND as far as hypermobility goes, in reality I am not THAT flexible. I will say that if you see me in a yoga class, you will likely think that I go all the time because I am basic yoga flexible. There is not a basic pose that I cannot do (except for pigeon on my right hip because that hip is tight). However, my secret is that I go to yoga on average probably one time per month. What?! How can I ALWAYS palm the floor without bending my legs, if I’m not practicing stretching everyday?
Well, turns out that if you have hypermobility, you can do that. Yay!? Now, don’t go celebrating or getting jealous at my near perfect downward facing dog. What does it mean to have hypermobile large joints?
It means that on a regular basis, I can get my large joints (knees, elbows, shoulders, ankles) off track. If this happens over and over (think walking with your kneecap moving slightly off track each step), then the muscles that are taking up the slack for the weak ligament (ligaments, in my case, are where my affected collagen are located causing the ligaments to be stretchier than is helpful) become inflamed. Another thing that happens is that if my muscles get too strong in one place and weak or not balanced in another, my poor stretchy ligaments cannot hold my joint in the correct place. This happens regularly to my shoulder joints. But more on that later.
Basically, I learned that I am not crazy. I am not making stuff up. I do not heal as fast as others, which is why I cannot follow as rigorous of a training schedule. I have to give myself time to heal between workouts, etc. So, yes, running two times per week is all I can do. Yes, strength training two times per week is great! Putting a cycling or yoga class in another day will work. AND YES, taking that extra day off if my PTT’s are hurting is fine. I’m doing it all in the right way. Listening to my body is the only way to go.
So, here’s to hypermobility. Thank you for letting me know that I’m not crazy and training slowly is okay.
Update on Spring 5/29/15
Posted by admin in Training (running, cycling, etc.), Try This! on March 30th, 2016
As I get ready for my grand summer of training, I figure I should reflect on what has been happening with regard to run training, bike training, and how the Whidbey Island 10K went.
So, my training for Whidbey was not super smooth, but I did get a PR! I beat my 2014 time by almost 1 minute 🙂
2014 10K results: total time 1:05:02
2015 10K results: total time 1:04:13.
I ran using the ProKinetics insoles. I had been having trouble with my Achilles tendon on my right leg and Posterior Tibial Tendons in both right and left legs on runs over 4 miles. I stopped once at 2 miles to do a cross friction rub (by the way, awesome way to trick your brain into releasing tendons or muscles!), again at 3 miles, then approximately every .5 miles until the end of the run – more frequent stops if uphills are involved. However, in the race I ran through the pain and made it the entire race without stopping, which is how I got my PR.
After the race, I have not been able to run without pain – anything over 2 miles. Did not stop me from trying to maintain a running regime
Also, side note:
I took the extra 3mm build-ups that come with the ProKinetics and put them in my bike shoes (that are clipless), and suddenly, I felt that I could actually put my big toes down in my shoes. In addition, my knee quit “wobbling” when I pedal. Kind of like magic. More on that later….
Now, I am back in physical therapy. More changes, Brian has moved onto an adventure through Ecuador – I hope he starts a blog! So, this week I worked with a new PT because the burning in my calf got to be very bad, and a massage made it very apparent that I have an inflamed soleus. Really terrified of rupturing my soleus. Nasty little muscle to heal.
Turns out that it is my insertion point for my Achilles tendon that is inflamed. So, no running. Lots of stretching and some exercises. And have to keep my head up. Hardest part. Not motivated to do the exercises because they are the eccentric motion that I have done before and not felt a lot of benefit. Bleh. Have to get going, but really sad.
Why injured? Overuse….I ramped up too fast, again. Smart training is key. More research and a plan needed. Definitely should have a plan.
I’m BAAACK! The Next Phase Plan and a Half-marathon!
Posted by admin in Appointments, Try This! on February 1st, 2015
It has been a while since that second triathlon (a.k.a. my last post). In that time, I have finished 4 sprint triathlons, one 10K and two 200 mile bicycle rides (Seattle to Portland (STP) and Ride from Seattle to Vancouver and Party (RSVP))! The reason that all of my triathlons have been sprint distance is in large part due to my run. Specifically, my Posterior Tibial Tendon (PTT) continues to give me pain in distances longer than 4 miles.
Here’s the puzzle: last year in May of 2014, I trained up to and ran a 9 mile training run, which is the longest distance I have ever completed, and I did it without pain. How? I have no idea, and it didn’t last long because quickly after that run, I upped my training with a sprint focused run group with the goal of speeding up my runs and increased mileage on the bicycle rides to accommodate the upcoming STP. Thus, I ended up in the Physical Therapists office with inflamed PTT. Needless to say, I did not complete the sprint speed training nor have I run 9 miles since.
So, why start the blog again? Because on my last visit to Brian Crosier, my Physical Therapist, he unlocked two final pieces to my puzzle, I think, and I want to document this next part of my journey.
In December 2014, I had started training up to a half-marathon, the Whidbey Island Half-Marathon on April 19, 2015, from 2 mile runs. All was great until I started running 3.5 miles and my PTT got inflamed. I also started to feel my tight right hip tighten even more. Hip tightness is a new thing that started over the summer after my STP ride with my untried new awesome carbon fiber frame bicycle, but I can tell you that story another time.
S0, I entered Brian’s office with mildly achy PTT and a fairly tight hip. As he was trying to figure out how to help me since I had already been through PTT treatment, and I was already applying the techniques he had taught me over the summer, he discovered an immobility that he had not considered treating before: my mid-foot.
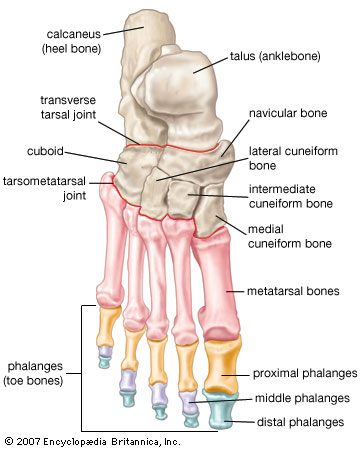
So, after Brian got the foot model, much like the picture above, he began by telling me about the three arches in the foot. There is the major arch that everyone knows about, then there is an arch on the outside of your foot between your heel and your midfoot, and finally, your toe knuckles are supposed to be an arch, but most people’s are flat and not arched at all. Hmm – I’m definitely in the flat toe knuckles camp: no surprise there.
He then added that my left big toe knuckle cannot touch the ground. I laughed and told him that my left big toe knuckle touches the ground every day 🙂 He responded by using the foot model to explain that on my left foot, my main arch compensates a lot for immobility though the mid foot or the navicular bone and the cuneiform bones, meaning it flexes or “falls” in order to allow my left big toe knuckle to touch the ground because those bones do not flex enough on their own. Consequently, the Posterior Tibial Tendon attaches to the navicular bone, which means that my PTT is already being stretched out everytime I flex my arch.
Whoa! What? When Brian told me this, so many issues that I have been having my ENTIRE life began to fall into place. I have always felt like I walk on the outside of my feet, and I have these weird outer foot calluses to prove it. Also, Brian had been coaching me to land “flat” with my feet (i.e. land mid foot with by toe and outer foot touching at the same time) because I land on the outside of my feet then roll in, which puts a lot of pressure on the PTT since it is in charge of the downward/flex motion of the big arch. Well, I have been trying to land “flat” since summer 2014, and I was not feeling very successful. Guess why – I can’t. I physically cannot get that big toe on either foot (the left is worse, but the right foot suffers as well). Finally, when I ride my bicycle, even after a fancy fitting with the spacers placed to help get my knee in the correct place, I always felt that I could not get my big toes down inside the shoes. Of course NOT! I felt so much better knowing that despite my trying and failing, it was a mechanical restraint.
But with me, I’m not satisfied with just the why. I want to know the next step – how do I correct this? Of course, Brian did not disappoint! He had invented a stretch for those small, largely immobile bones of the midfoot. Â I will post a video soon with details on how to do this stretch. For now, know that after the first stretch with Brian, the tops of my feet were sore (both left and right) for two days, and the stretch is not very big. It is just that that part of my foot had never really been stretched.
Another component of the foot issue is how to get the big toes on each foot to touch the ground while still maintaining as much subtalar neutral (ankle being neutral and arch not fallen) as possible? This took convincing – Brian suggested ProKinetics® insoles that have 3mm build-up under the big toe area on each foot (see red part on the photo below). As most of you know, if you have read very much of my blog, I do NOT like inserts of any kind. After working for over a year to get out of prescription orthotics, I am not very enthused about having to use any kind of inserts again. However, Brian made a compelling point: with these inserts, my feet could possibly be placed into a better position that would allow more natural functioning with less pressure on the PTT. Hmmmmm….why does he always make such good arguments?
So, I got the ProKinetics® Insoles. They have a 3mm build-up (in red) under the big toe as well as a removeable (yell0w) arch support. In addition, they come with an extra set of 3mm build ups (orange) in case you would like a 6mm build up.
ProKinetics Insoles
Since lots of my shoes are more minimal (Five Fingers and Luna Sandals), I also purchased a really cool adhesive lift that you stick directly to the ball of your big toes called SoleMateâ„¢ Comfort MicroLiftsâ„¢. Very cool products.
I am still in the test phase of running with full insoles, but so far the first run has been good, and I wore theSoleMateâ„¢ Comfort MicroLiftsâ„¢ with my cycling shoes today and what a difference! I know what the bike fitters have been telling me about using my whole foot – I could actually do it! My inner thighs are going to be very sore since I can access their power now, too!

The picture shows how the SoleMateâ„¢ Comfort MicroLiftsâ„¢ look and adhere to your foot. Weird, but very effective. I will say that I wore them for my trainer ride on my bicycle, and I put them back on my feet after my shower and wore them for approximately 8 more hours. Around hour six, I could tell that the skin under the adhesive was getting  a little irritated. However, when I removed it I did not have any lasting redness or raw places. The website says that these can be stuck directly to the inside of the shoes, too. So, I’m going to try that to see how it works. Definitely adding the additional 3mm orange pieces to the bicycle shoes, though!
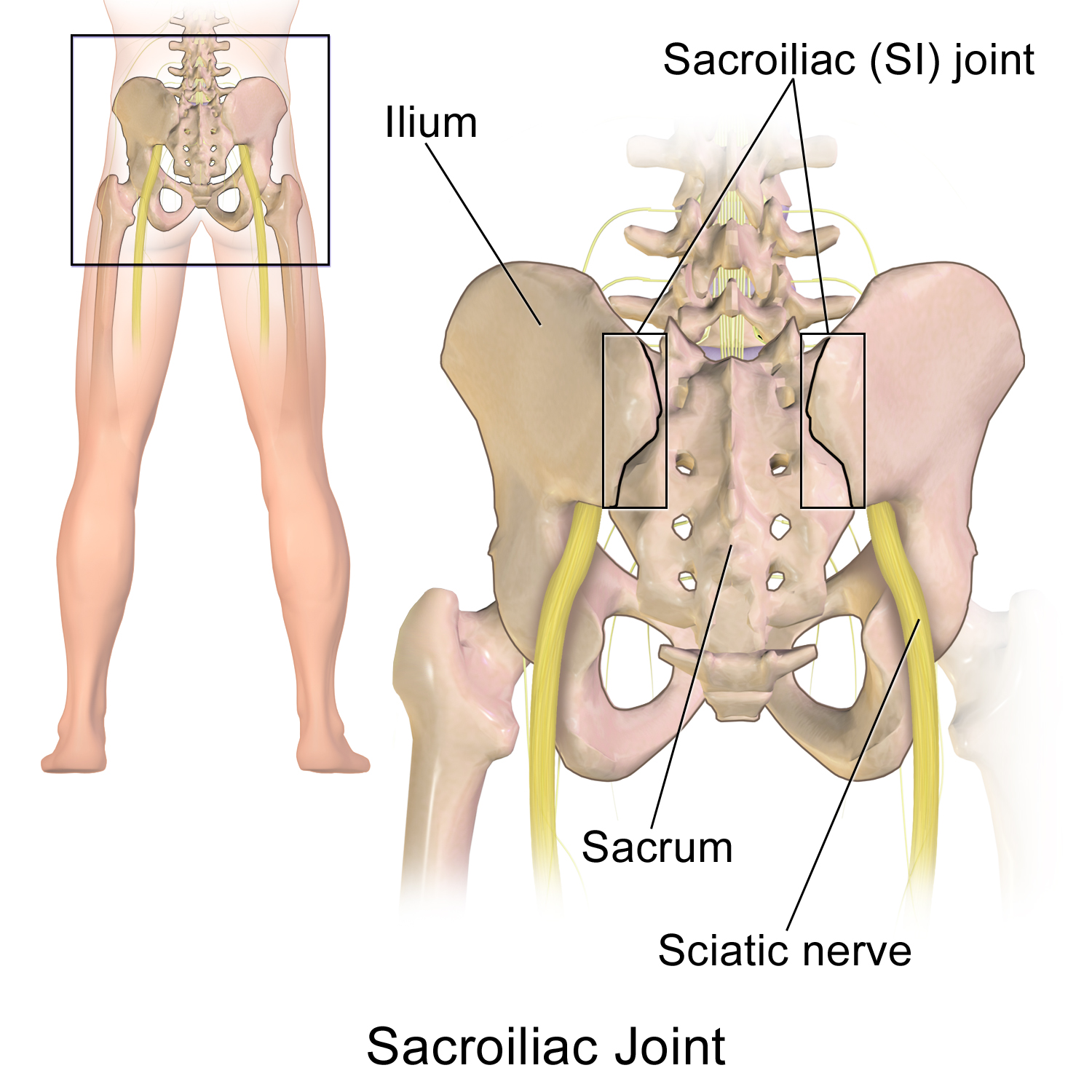
Part two: tight hip
The why – my Sacroiliac (SI) joint on the right side, as seen in the photo below, was tight, which was impeding my ability to do some rotation and other movements, and my hip muscles, specifically the gluteus minimus, were taking up the slack and ending up overworked and tight.Â
 Once again, bells were going off all over the place! YES! The SI joint was tight on the right side! Of course, a few years ago I had spent an entire summer using a lacrosse ball on the right SI joint when Brian had suggested that I tuck my tail bone when I run in order to use more core muscles and attain a more efficient running form. I had not really thought much about my tail bone once it had stopped hurting, but I had never really treated it. Well, SI joint, those days are done. I am not going to neglect you anymore.
Once again, bells were going off all over the place! YES! The SI joint was tight on the right side! Of course, a few years ago I had spent an entire summer using a lacrosse ball on the right SI joint when Brian had suggested that I tuck my tail bone when I run in order to use more core muscles and attain a more efficient running form. I had not really thought much about my tail bone once it had stopped hurting, but I had never really treated it. Well, SI joint, those days are done. I am not going to neglect you anymore.
The how on treating the SI joint? To have Dr. Larry, my wonderful Chiropractor, do his magic on the SI joint when I visit him and to re-start some tennis ball massages on the SI joint. Also, I have a massage therapist, Brad, who has been working on my right hip. He will be better able to attack the problem with the new information as well. Gotta love having a village to keep it all working smoothly!
So, this is the next phase – unlock mobility in my midfoot and loosen up the SI joint on the right side. I’m still signed up for that half-marathon in April, and I’m looking forward to the training! If I can find the right combo of mechanical advantage and training pace, I may just make that race! Stay tuned!
9/11/12 – A Momentous Day, PT and Chiropractic Work
Posted by admin in Training (running, cycling, etc.), Try This! on September 17th, 2012
On September 11th, 2001, I was still in graduate school at Georgia Tech. I had gotten up and was getting ready for an 8:30am class, while watching Matt Lauer and Katie Couric on the Today Show. All was well until I came back from another part of the apartment to find a burning, smoking building on the screen. At first, I thought it was a hoax. How could a building in New York City be burning? Then, Katie and Matt were taking turns trying to explain what was going on when an object hit the second World Trade Center tower. “What is happening???” I kept asking in my head as Katie and Matt continued to work on explaining a horrific scene.
On this day, my cousin also had her 16th birthday. It was not the day she would get her driver’s license, though.
This year, I had a pretty big day with a Chiropractic appointment and a physical therapy appointment.
First, I went to Dr. Larry’s. I was having a pain in my right glute max, and my thought was that it might be L5. Dr. Larry said that it sounded more like S1. So, he adjusted, and it felt great! He also did the usual neck, back hips and ankles with a little right wrist for good measure.
Then, I headed down to see Brian for physical therapy. I was wondering if it was too much to do these two things on the same day, but then I figured, why not?
I told Brian about Dr. Larry’s verdict on the S1 adjustment, and Brian said that it made a lot of sense b/c the S1 is the nerve that controls the Posterior Tibial Tendon, among other tendons in the foot. So, if you’re S1 nerve gest severed, then your Posterior Tib Tendon will not work. Hmmmm, interesting. Does that also mean that if your s1 vertebra is out of alignment, then your Posterior Tibial tendon will have a difficult time working to its fullest capacity? Good question. I do not have the answer, but it certainly does make one think.
Brian worked on ASTYM for the posterior tibial tendon and the back of the calf. Still crunchier on the right than the left. Also, I was more tender from the Iron Girl 5K. He then had me do a calf warm-up (downward dog), the World’s Greatest Stretch (coming soon), and a few running warm-up moves. These running warm-up moves included learning to hop softly for approximately one minute. The “soft hops” are shown in this video by Sanatan Golden, a PT in Portland, OR, who helps to produce “Minimalist Mondays” videos and clinics.
We then practiced foot “lifts,” which are a warm up where you try to lift your foot rather than hop from foot to foot in order to prepare for a run.
Finally, he had me run on the treadmill. This is going to be an ongoing exercise, too. Despite my reservations and rebelling against running because I am terrified of continually reinjuring myself – you know the dance: two steps forward, three steps back. However, when asked to run for a camera, I cannot say no. The following video is from Sept. 4, 2012.
Note: I had no idea Brian would suggest running that day. So, I was not dressed for success in running. Also, the creepy slow voice is Brian asking me if I am relaxed in the second video. I have some serious video editing skill deficits to overcome in the future.
I have not put the later videos together, but I might just do a video post later. For now, check this out!
In the left-most video or Video #1, I am trying very hard to remember all of the steps to running barefoot: tilt pelvis up, lift legs, head up, chest expanded, shoulders back, try to create a forward lean, etc. Notice that my legs do not always come up very far on the up swing (less than 90 degrees). In the right-most video or Video #2, Brian has showed me the first video, then told me to relax and think of being light, relaxed and quick. I also only worked on tilting my pelvis up (I had to think of something – what is this relaxed thing, anyway???).
Guess what? Relaxing and not worrying so much produced a better stride naturally. These videos were only a few minutes apart. Brian literally showed me the first video, talked about good things (thank you for doing that, I had enough negative self-talk going on for about four people at the time), and then added that I could just relax. Very well done, indeed as that second video shows. My legs swing up to 90 degrees, my pelvis is in a good place, and I might even be smiling.
Although this video is from last week, it mimics the video from 9/11/12.
So, don’t sweat the small stuff, and just relax!
9/6/12 – Physical Therapy and More!
On Thursday, I headed to PT. I wondered what we talk about that day!
They have an intern, which I love because it means that the Physical Therapist will explain what he is actually doing as he does the treatment. I do not always follow what is being said, but it is so fascinating. AND if I act interested, I get in on the explanation in layman’s terms. 😉
He was making an adjustment in one of the joints in my foot (tried to look this up, but there are so many joints that I cannot actually say which joint it was) in order to create space in the joint to help my dorsiflexion as that is the flexion that is inhibited on both of my feet and explaining the procedure to the intern. I was super fascinated, but the complex or rather the unfamiliar terms totally threw me off. It really does make me want to get a PT degree, but I’m not really interested in treating lots of different people in lots of different areas. I’m really only interested in feet.
Anyway, I learned how to do a scorpion stretch, a bridge with a leg lift that engages the core the same way that the core is engaged during a running stride, and three different ways to work the core without using the hip flexors. 1. Do a bridge on a stability ball and crunch up. By making the glutes work in the bridge, the hip flexors cannot work. Thus, only training the ab muscles and glutes. 2. Do crunches with your feet together and knees laying out to the side in a butterfly. In this position, the hip flexors absolutely cannot engage. 3. Squeeze a ball between your knees (this is what Melissa already has me do). By making the hip adductors work, the hip flexors are blocked.
Totally awesome!
Stay tuned for another aspect to my blog and more pictures and links to videos of these exercises and more!
8/30/12 – Physical Therapy Blows My Mind
Consider my mind blown. Completely.
I was talking to the ultimate choir today. I was told that there is a podiatrist who believes in minimalist walking/running. He lives in Portland. His name is Dr. Ray McClanahan. Wow! That took me a second.
Also, a physical therapist, Sanatan Golden, in Portland (might have a funny TV show based on stereotypes in that town, but I believe Portland is looking like a good city right about now) who hosts a web YouTube called “Minimalist Mondays. ”
Next, Brian showed me his very own foot treatment. Practicing what he preaches. Doing his own exercises.
Finally, he read my blog. Not all of it, but some of it.
Wow. Mind blown. Thanks, Brian.
Actually, that wasn’t all. I mention that my knee is super crunchy when I do the active hamstring stretches, and he pulls out a mini plunger and some of the ultrasound goo to help make a good suction area. Before we use these things, he shows me how to move my kneecap around to help mobilize it. Then, after noticing how it likes to move down, but not so much up and especially not up and to the right, he squeezes the goo out and begins to plunge my knee. It’s like having traction done on your kneecap, and it feels amazing. He explained that this would help to lubricate the joint as well as encourage more circulation to the area. There was also a bit about the neurological factors involving isometrics and cramps, but it is late. More on that, perhaps later.
Next, he ASTYM’ed my ankle and calf muscles. The right heel where the Achilles Tendon attaches hurt a lot more than the left. Really, everything on the right side hurt more and was crunchier (definitely a scientific term).
He showed me how to massage my tendons and muscles between my big toe and the other toes. This increases the big toe’s flexibility and ability to move out and increase the width of my foot. Oh, I guess I forgot to mention that the wider the foot, the better! Take that shoe industry! Where are my WIDE toe boxes???
I also learned how to stretch the top part of my foot and use a baseball to help increase the flexibility under my forefoot or help the arch that should be there redevelop.
So, now I’ve got 5 exercises!!! I think we’re getting somewhere 🙂
8/23/12 – New Physical Therapist
I showed up to the new physical therapist not too sure what to think or do with myself. I always have somewhat of a haughty speech prepared. You know, I have this foot problem. It’s always been a problem. I know SO much about it. -Insert diarrhea of the mouth here.-
Over the past few months, I’ve been thinking/analyzing my approach to transitioning to minimalist. Specifically, I’ve been pondering how I present myself to others when talking about the strengths and benefits of going barefoot. And I decided that I sounded like a crazed advertisement on the Home Shopping Network or something.
Well, that’s not the look I’m going for. As a matter of fact, that’s quite the opposite.
So, when I sat down with Brian Crosier, the PT at Madison Physical Therapy, I decided to be a little more tactful. I let him ask questions, and I did throw in the extras like the club feet and a little bit of history. Of course, I also plugged my blog.
He then did the usual tests. This time, the numbers:
Ankle Dorsiflexion (ability to bend in ankle) in knee extension (knee out straight): L 4 R 7
Ankle Dorsiflexion (ability to bend in ankle) in knee flexion (knee bent): L 6 R 9
And I quote, “These numbers suggest you have both talocrural joint stiffness, and soft tissue restrictions limiting your ankle dorsiflexion range of motion. This will result in your posterior tibialis needing to engage early in your stride, one of the several things that will lead to increased loading of that tissue.” Cool!
Knee to wall test (consequently, Travis did this test with me in one of my final appointments with him- not sure what those numbers were. I’ll look it up and edit)
Left: 8.5cm (cheating by allowing my talus or arch area to drop and make up for the stiffness), without talus dropping (Brian pointed out the cheating and directed me to not let the arch drop resulting in a smaller number than the right foot!), 7cm.
Right: 8cm
Goal: 10+cm on each foot
He then told me to do two exercises. TWO exercises? Is that it? I mean, I’ve got healing to do. Isn’t there more?
“No,” he replied. He then said very matter of factly, that it was obvious that I like to overdo it. I mean, I was walking right back into PT. Touche.
So, I have a specific exercise for the posterior tibialis and an active hamstring stretch. 🙂
12/11/11 – Updates and Procrastination….
Posted by admin in Reflections, Try This! on December 11th, 2011
When I left off, I was working on the 5K. However, as I reflect on my performance in Oct and Nov of the past two years, I find that life has a way of really getting in the way during these two months. I am now recovered from a very busy and emotionally draining Oct., and November’s celebrations and holiday are done, too 🙂
Now, back to work. I realized that I have yet to get my running videos from Travis. I took him a thumb drive that was too small (I think it is about 10 years old – do any files equal less than 128MB anymore?), and that was the last time I tried to get the videos. Since I have reminded myself, I will focus on getting the videos from him this week or next week when my winter break from work starts (Hooray!).
With the videos I will begin a new regimen of running. The running is very difficult in VFFs in the winter due to the cold and wet conditions combined with the Raynaud’s Phenomenon, which causes my fingers and toes to go numb with the slightest chill. I find that running on wet pavement in the winter causes my toes to go numb really quickly, which leaves my feet feeling like big blocks of wood that are propelling me along. I will say that when I ran a 5K (more like walk/jog) on Thanksgiving day, my feet were numb within 1/4 mile, but at mile 2, the feeling began to return to my toes as my body heat increased. It was a very pleasant finding that I have been unable to compel myself to replicate :-/
I am continuing to work with Melissa, and we have had to scale back my workouts due to my lack of motivation (read: I do not go to the gym unless she is with me). I am also in the process of changing to a gym that has a TRX device. My first TRX workout was last week, and it was such an amazing change of pace. I will write more on the device later. To balance out the TRX workout with my regular workout (the only way to workout lower body large muscle groups is squats and lunges on the TRX, and my right knee is currently rebelling against those two moves), I am doing a regular non-TRX workout this week. I did go to the gym one time between my workouts with Melissa last week due to my interest in the “new” TRX workout. Yes, it was rather like a kid with a new toy. My new plan is to workout once between training sessions with Melissa followed by a yoga class the next day to help increase flexibility. If I can get back into the workout habit, then Melissa can up my routine, and I can start rebuilding strength. Yay!
Motivation is slowly coming back. The biggest factor is that I just turned 35, and my thighs look more like 35 year old thighs than 25 year old thighs, which is not how I want my thighs to look. I mean Cher looked awesome at 65, but I think I read somewhere that she spent 3 hours in the gym each day. I guess there’s something to look forward to. At least I won’t be bored in retirement, and I could wear a thong leotard and dance on a Navy ship with all of the sailors. Now, that’s a good retirement plan…..
9/13/11 – PT, My Jaw Story, and a Workout!
I am moving toward a goal of posting more, again, on the blog 😉
So, today was a visit to Travis about my right shoulder. I originally started visiting him concerning an inflamed biceps tendon, but since then, it has changed to more a slightly sore infra-spinatus. The cause seems to stem from my lifelong habit of clenching my jaws together,which I am also seeing a different specialist for.
Anyway, over the weekend I had to get a massage to relieve my shoulder pain due to excessive clenching, which causes a chain reaction of my levator scapula getting tight and causing a downward rotation on my shoulder blade, which then causes the rest of the rotator muscles- that are already a little too weak – to work super hard to get the upward rotation on the shoulder blade. The end result is an inflamed small muscle or tendon in my shoulder and a very tight neck and top of shoulder area. Argh.
The massage enabled me to run the 5K Iron Girl on Sunday, but by today, I was already super tight again and feeling some discomfort in my shoulder. Travis, being the incredibly knowledgeable PT that he is, did a very specific massage, which loosened up the muscles enough so that we could actually do some exercises. He, then, took it fairly easy on me due to the inflammation of the new area.
I also told him what I had learned about my jaw from the specialist at UW. It goes something like this:
I broke my only crown, which I had had for 10 years, in January of this year and had it replaced in February. After the replacement is has hurt and continually extruded (or pushed up). My dentist filed it down three times before determining that it was probably something more serious and sent me to an endodontist due to my long tooth roots.
Cut to endodontist: She determined that I had a cracked tooth, which had been held together with the old crown, and opened up with the new crown, which equals a ROOT CANAL! Yay! The root canal was supposed to solve the problem and stop the tooth extrusion.(She also measured my tooth roots b/c I was wondering how long they were and why they were considered so long. It turns out my tooth roots are 25mm long, and a normal tooth has roots approx. 22mm long. And now you know….)
Note: this whole time I am wearing my night guard religiously each night. My night guard is basically a mold of my teeth with some kind of plaster built up on the front part to keep my teeth from touching in the back. The only teeth that touch are the front ones, and boy can I feel it in the morning on the front teeth when I’ve had an exceptionally clench-filled night.
Well, the root canal on August 16th did not stop the tooth from continuing to extrude. My endodontist even did a file down to help ease the discomfort about one week later.
In the mean time, I set up an appointment with the TMJ specialist at UW. I explained the whole process to him, and he immediately was impressed that I knew how long my tooth roots were. 🙂 I’m such a nerd sometimes. Anyway, the result of the dissertation I made and the observations he made were that my night guard was causing the tooth to extrude. WHAT?! The freakin’ night guard that I dislike anyway is causing this entire catastrophie?! ARGH!
Here’s what was happening. He said that it is well known and thought of that a tooth on the top of the mouth without a tooth to oppose it on the bottom will overtime extrude because it does not have any force to oppose it and keep it in place. It is still known, but not really thought of (as in it is not the immediate conclusion) for bottom teeth, which is what my tooth is. So, my bottom tooth was inflamed, which means that the bone is building up around the root to help protect it, and the tendon surrounding the roots are working overtime to try and get the inflamed object to go away (i.e. extrude). Normally, after the root canal the tooth has a chance to calm down and stay in place b/c at some point in the day, it will hit the opposing upper jaw tooth and stay in place. However, due to my unfortunate nightguard, my back teeth NEVER touched, and my poor inflamed tooth was able to continue to push out each and every night.
He told me to throw out my nightguard because he was going to give me a new one (the temporary is a simple sports self-mold model – this thing is huge, but all of my teeth can touch the bendy plastic substance it is made out of). His theory was that with the touching of the teeth on something, the back tooth would begin to intrude, which it has, happily, done! Woohoo!
The second part of my treatment is all behavioral, i.e. I have to change my clenching habits during the day. I also learned that your teeth do not actually touch when your jaw is in a resting position. Many of you already knew that – lucky for you. I had no idea! I’ve been clenching my whole life thinking I was relaxed! No wonder my shoulders are like rocks.
So, my homework is to continually remind myself to relax my jaw – keep the tongue resting behind the front teeth while the teeth remain slightly apart to give the jaw joint space. I have been completely amazed by how often and how severely I clench during the day, even. It’s crazy! I especially clench during upper body (specifically shoulder) exercises. I also clench when I run, get really stressed at work or just sit and read facebook. My day now consists of me checking the status of my jaw and relaxing constantly.
I told Travis all this today, and he also added that the levator scapula is very tight possibly due to weakened multifidi on the C1-4 vertebrae. So, I now am working in pushing my tongue against the roof of mouth to fire those extremely tiny muscles along my spine. Woohoo! I’m just afire with crazy crap to keep up with.
Travis also finished analyzing my running video that we made several weeks ago. Due to the file size, I will not have it in my possession until I am able to get a thumb drive to him to download them. I will save his findings for the video.
I also ended my day with a workout from Melissa. Woohoo! I’ve gotten it all in this week. I’m going to try and run tomorrow as it will be day three after the race, which should be enough time for recovery, maybe.
Things are very exciting right now. I really believe if I can tame my jaw clenching, then I will see a huge reduction in my various discomforts and ailments. Never underestimate how connected the entire body is.
p.s. Travis measured the flexibility of the achilles tendon by measuring how far away from the wall I can stand and touch my knee cap to the wall. I’ll explain why in the video post, but for now the numbers – so I don’t forget them.
The right foot (big tow) was 5.5cm from the wall, and the left foot (big toe) was 7cm from the wall. These numbers are new measurements that I look to improve to the goal of 10cm for each foot over time.
2/18/11 – Physical Therapy Before the Ski Trip – Different Therapist
Based on Travis’s recommendation that I come back in before I go on my ski trip so that I get some work done to loosen the tissue around my patella and learn how to tape, I had to make an appointment with a different therapist. At Seattle Physical Therapy, there are only three therapists. So, I have definitely seen all of them at work at some point.
I had a 7am appointment with Jeff, who was very thorough in his investigation. He found that my right VMO (little quad muscle on the inside of the knee) was slightly less firm than the left, which he hypothesized meant it wasn’t firing as effectively. Also, he said that I most likely wasn’t using my pelvic floor muscles (if you’re female, think Kiegle exercise) when lifting or using the leg.
So, he tested these, and sure enough, I had a drop in the right hip when, laying on my back, I simply lifted the right leg straight into the air. Ah, those lazy pelvic floor muscles.
Thus, I ended up with two more exercises (one for the VMO – turn the right foot out and lift the leg straight up with the left leg bent and supplying support – and one to teach me to use the pelvic floor muscles while simply raising one leg at a time straight up in the air.), which both proved to be insanely difficult. Shouldn’t I be able to lift my legs???
Jeff also taught me a different way to tape, which worked as well, and I was off to ski!